
Retinoblastoma Management Case 3: From Brenda Gallie, MD
Dear Board Members!
The Eye Cancer Network thanks Dr. Gallie for sharing her interesting management case. We further thank the respondents for taking the time to share their thoughts, recommendations, and opinions.
Bilateral Retinoblastoma in a 6-day old, Dr. Gallie requested suggestions as to treatment options to optimize visual outcome without risk to this 6 day old, 37 week gestation, baby with bilateral familial retinoblastoma.
The Eye Cancer Network thanks Dr. Gallie for sharing her interesting management case. We further thank the respondents for taking the time to share their thoughts, recommendations, and opinions.
Bilateral Retinoblastoma in a 6-day old, Dr. Gallie requested suggestions as to treatment options to optimize visual outcome without risk to this 6 day old, 37 week gestation, baby with bilateral familial retinoblastoma.
We received the following responses
Thank you for submitting Brenda's case. I just happen to have a similar case last week in a child born at 38th week of gestation with a low birth weight of 2.2kg. She had a bilateral retinoblastoma group B (tumor of 2 dd right in the papillo-macular bundle). The option taken was to gently heat the tumor by diode-laser mediated thermotherapy (I applied 300mW for 8 minutes) with no visible change. This will save a couple of weeks before applying chemoreduction. My experience is that axons are partially preserved by applying regular thermotherapy as exemplified by one of my first thermochemotherapy patients who had a tumor in the papillo-macular bundle in an only eye and a final visual acuity of 0.3 at 11 years of age. - Francis Munier
I would suggest low power TTT associated with a pre-TTT intravenous carboplatin injection Best regards ! - Patrick De Potter
Try chemotherapy alone, without adjuvant laser. In our London series it produces sustained control in 25% of eyes. If it fails, salvage chemo/laser may save the eye though the vision won't be as good. In our series, there is no evidence overall that primary chemotherapy with adjuvant laser saves more eyes than chemotherapy alone with chemo/laser salvage for failure. I'm sure that Brenda will exclude lens- sparing external beam radiotherapy on the grounds that it will risk the child and at six days of age I would have a lot of sympathy with this view. Nevertheless, speaking as someone who has treated many children in both ways, the visual results in children like this one were undoubtedly better overall in the era of external beam radiotherapy and we hope to support this assertion with data in the near future. I still do believe that some children over a year old may actually be better treated by radiotherapy. It is of note that the majority of people who discount this approach outright have no experience of the radiotherapy era. - John Hungerford
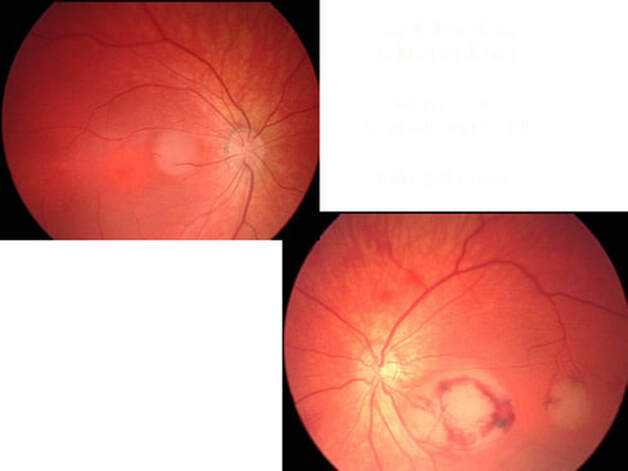
Thanks for posting Dr.Gallie's case on the website. The child appears to have bilateral multifocal retinoblastoma with active tumors in both eyes. The left eye shows sub foveal hemorrhage, which will compromise the vision either way. The right eye shows a tumor on the papillomacular bundle close to the fovea. The age of the child appears to be a confounding factor as far as chemoreduction is concerned. The other issues being location of the tumor and family history of retinoblastoma, which increases the risk of other neoplasms in this child. We have treated two children with triple drug chemoreduction and focal treatment, which were seen immediately after birth with large tumors. The children were treated with a lesser dose of chemotherapeutic agents than conventional treatment. The tumors responded well to chemoreduction and 2-4 cycles were used. Both children however needed additional local treatment. One child is now 1 1/2 years old and does not show any serious side effects as yet. The other child was however lost to follow-up. If the tumor in the right eye regresses only with chemoreduction and no any local treatment, that would be ideal but considering the age and family history, the child may need chemoreduction for a prolonged duration, with its attendant risks. These issues may have to be sorted out with the parents of the child. The left eye may be treated with local treatment after chemoreduction as this eye will anyway have suboptimal vision. If Dr.Gallie would like to know the dosage of the chemotherapeutic agents used, I can request our oncologist for the same. The other option for the right eye could be photodynamic therapy, which can spare the fovea to some extent. However, delivering photodynamic therapy would be difficult in a recumbent child and toxicity data on verteporfin in a child of this age is not readily available. PDT (if the risks are acceptable) may be used after chemoreduction to decrease the chances of foveal damage. Thank you - Dr P Mahesh Shanmugam
The case you present is indeed challenging concerning the visual outcome of this baby. We have had a little bit similar familial case and we decided to treat with chemoreduction 3 courses to minimize the tumor, followed by thermochemotherapy until an atrophic scar has developed. The laser treatment should be administered very gently with low energy to start. Furthermore, it is of equal importance to prescribe amblyopia treatment (occlusion alternately). This would be our management in Amsterdam. Good luck, Saskia Imhof
Warm regards,
Paul T Finger, MD, FACS
The Eye Cancer Network
DISCLAIMER: Postings on The ECN Mailing List are strictly the opinions of the authors. The ECN and its sponsors assume no responsibility for the accuracy of the information, nor do they assure the safety or effectiveness of any clinical recommendations in these postings.
Receive the latest news and opportunities from The Eye Cancer Foundation. Please fill out the form below.
Thank you for submitting Brenda's case. I just happen to have a similar case last week in a child born at 38th week of gestation with a low birth weight of 2.2kg. She had a bilateral retinoblastoma group B (tumor of 2 dd right in the papillo-macular bundle). The option taken was to gently heat the tumor by diode-laser mediated thermotherapy (I applied 300mW for 8 minutes) with no visible change. This will save a couple of weeks before applying chemoreduction. My experience is that axons are partially preserved by applying regular thermotherapy as exemplified by one of my first thermochemotherapy patients who had a tumor in the papillo-macular bundle in an only eye and a final visual acuity of 0.3 at 11 years of age. - Francis Munier
I would suggest low power TTT associated with a pre-TTT intravenous carboplatin injection Best regards ! - Patrick De Potter
Try chemotherapy alone, without adjuvant laser. In our London series it produces sustained control in 25% of eyes. If it fails, salvage chemo/laser may save the eye though the vision won't be as good. In our series, there is no evidence overall that primary chemotherapy with adjuvant laser saves more eyes than chemotherapy alone with chemo/laser salvage for failure. I'm sure that Brenda will exclude lens- sparing external beam radiotherapy on the grounds that it will risk the child and at six days of age I would have a lot of sympathy with this view. Nevertheless, speaking as someone who has treated many children in both ways, the visual results in children like this one were undoubtedly better overall in the era of external beam radiotherapy and we hope to support this assertion with data in the near future. I still do believe that some children over a year old may actually be better treated by radiotherapy. It is of note that the majority of people who discount this approach outright have no experience of the radiotherapy era. - John Hungerford
Thanks for posting Dr.Gallie's case on the website. The child appears to have bilateral multifocal retinoblastoma with active tumors in both eyes. The left eye shows sub foveal hemorrhage, which will compromise the vision either way. The right eye shows a tumor on the papillomacular bundle close to the fovea. The age of the child appears to be a confounding factor as far as chemoreduction is concerned. The other issues being location of the tumor and family history of retinoblastoma, which increases the risk of other neoplasms in this child. We have treated two children with triple drug chemoreduction and focal treatment, which were seen immediately after birth with large tumors. The children were treated with a lesser dose of chemotherapeutic agents than conventional treatment. The tumors responded well to chemoreduction and 2-4 cycles were used. Both children however needed additional local treatment. One child is now 1 1/2 years old and does not show any serious side effects as yet. The other child was however lost to follow-up. If the tumor in the right eye regresses only with chemoreduction and no any local treatment, that would be ideal but considering the age and family history, the child may need chemoreduction for a prolonged duration, with its attendant risks. These issues may have to be sorted out with the parents of the child. The left eye may be treated with local treatment after chemoreduction as this eye will anyway have suboptimal vision. If Dr.Gallie would like to know the dosage of the chemotherapeutic agents used, I can request our oncologist for the same. The other option for the right eye could be photodynamic therapy, which can spare the fovea to some extent. However, delivering photodynamic therapy would be difficult in a recumbent child and toxicity data on verteporfin in a child of this age is not readily available. PDT (if the risks are acceptable) may be used after chemoreduction to decrease the chances of foveal damage. Thank you - Dr P Mahesh Shanmugam
The case you present is indeed challenging concerning the visual outcome of this baby. We have had a little bit similar familial case and we decided to treat with chemoreduction 3 courses to minimize the tumor, followed by thermochemotherapy until an atrophic scar has developed. The laser treatment should be administered very gently with low energy to start. Furthermore, it is of equal importance to prescribe amblyopia treatment (occlusion alternately). This would be our management in Amsterdam. Good luck, Saskia Imhof
Warm regards,
Paul T Finger, MD, FACS
The Eye Cancer Network
DISCLAIMER: Postings on The ECN Mailing List are strictly the opinions of the authors. The ECN and its sponsors assume no responsibility for the accuracy of the information, nor do they assure the safety or effectiveness of any clinical recommendations in these postings.
Receive the latest news and opportunities from The Eye Cancer Foundation. Please fill out the form below.
