
Pigmented Juxtapapillary Tumor Case 13
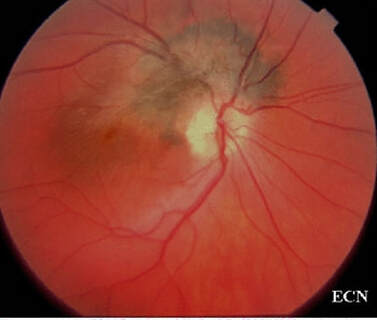
Digital funduscopic image of the pigmented juxtapapillary tumor
|
Tumor Board Presentation from Paul T. Finger, MD
Subject: Unknown Date Posted: October 21st, 2003 Dear List Members We have a interesting case and would like to get your comments. Case This 28 year old female noted 6 months of progressive loss of vision in her right eye. Her vision is 20/40, the anterior segment is normal, and there is no afferent pupillary defect. Ophthalmoscopy revealed a pigmented subretinal tumor with traction maculopathy. The apex of the tumor revealed intraretinal vasculopathy. The optic nerve appeared displaced and pale in the meridian of the tumor. There was no overlying vitritis. |
Ophthalmoscopy revealed a pigmented subretinal tumor with traction maculopathy. The apex of the tumor revealed intraretinal vasculopathy. The optic nerve appeared displaced and pale in the meridian of the tumor. There was no overlying vitritis.
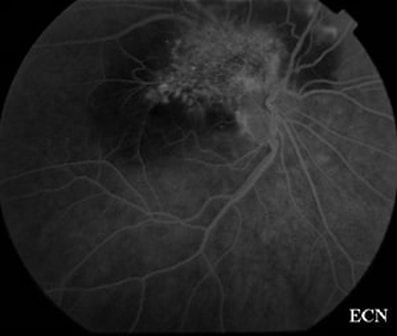
Early flourescein angiogram of the juxtapapillary tumor demonstrates intrinsic vascularity
|
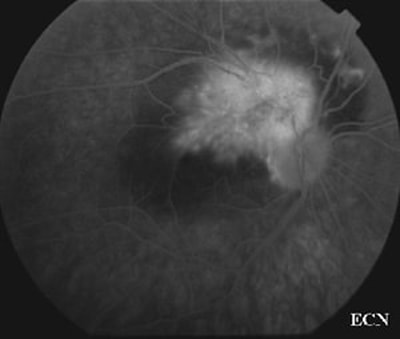
A late fluorescein angiogram demonstrates vascular leakage with confluent flourescence
|
A late phase angiogram reveals diffuse intraretinal leakage limited to the area of hypervascularity.Early phase fluorescein angiography reveals a pattern of intraretinal microangiopathy with leakage. The rest of the tumor blocked fluorescence.
|
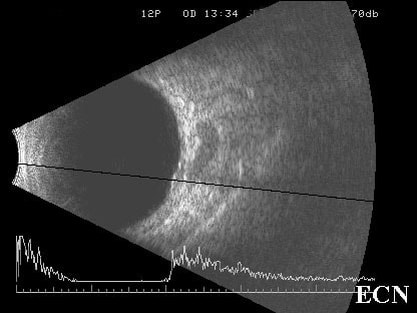
The tumor appeared to be moderately low reflective. Follow up computed tomography of the orbit revealed no evidence of extraocular extension or optic nerve invasion. A systemic medical work up including uveitis studies were all negative. What will be your approach in this case?
|
|
Responses From ECN Members
Dear ECN List Members,
This 28 year old female has a combined hamartoma of the retina and RPE.
I would order an optical coherence tomography (OCT) which may help explain the recent onset of VA decrease.
I would not recommend a biopsy.
If traction on the macula is demonstrated by OCT (due to excessive glial proliferation) then a vitrectomy may be considered. However, I would lean towards observing this case.
Best regards,
J. Fernando Arévalo, MD
[email protected]
Dear ECN List Members,
This 28 year old female has a combined hamartoma of the retina and RPE.
I would order an optical coherence tomography (OCT) which may help explain the recent onset of VA decrease.
I would not recommend a biopsy.
If traction on the macula is demonstrated by OCT (due to excessive glial proliferation) then a vitrectomy may be considered. However, I would lean towards observing this case.
Best regards,
J. Fernando Arévalo, MD
[email protected]
Dear List Members,
This lesion looks to me like a combined hamartoma of the retina and RPE.
I would observe this lesion and not perform a biopsy.
Best regards,
Pamela P. Rath, MD
[email protected]
This lesion looks to me like a combined hamartoma of the retina and RPE.
I would observe this lesion and not perform a biopsy.
Best regards,
Pamela P. Rath, MD
[email protected]
Dear List Members,
The case is indeed very interesting. The lesion is rather flat, hyperpigmented, and has associated orange pigment. The surface retinal vascular changes are most likely secondary to compressive effects of the lesion on retinal branch veins. On the ultrasound there are two components: a small choroidal and large extrascleral lesion. The lesion most likely represents a juxtapapillary choroidal melanoma with extraocular extension. It is unusual, but small tumors can behave like that especially in the juxtapapillary location. An MRI with surface coil, fat suppression, and Gadolinium enhancement is my recommendation, it is more sensitive than CT for revealing small melanin containing orbital tumors. If the MRI is positive for tumor, exploratory orbitotomy with possible enucleation ( if brown mass is seen) should be considered. Although tempting, incisional biopsy of the orbital lesion perhaps is best avoided. Transvitreal biopsy is likely to have low yield due to small size of the tumor. Would be keen to know the outcome.
Best regards,
Arun Singh, MD
[email protected]
The case is indeed very interesting. The lesion is rather flat, hyperpigmented, and has associated orange pigment. The surface retinal vascular changes are most likely secondary to compressive effects of the lesion on retinal branch veins. On the ultrasound there are two components: a small choroidal and large extrascleral lesion. The lesion most likely represents a juxtapapillary choroidal melanoma with extraocular extension. It is unusual, but small tumors can behave like that especially in the juxtapapillary location. An MRI with surface coil, fat suppression, and Gadolinium enhancement is my recommendation, it is more sensitive than CT for revealing small melanin containing orbital tumors. If the MRI is positive for tumor, exploratory orbitotomy with possible enucleation ( if brown mass is seen) should be considered. Although tempting, incisional biopsy of the orbital lesion perhaps is best avoided. Transvitreal biopsy is likely to have low yield due to small size of the tumor. Would be keen to know the outcome.
Best regards,
Arun Singh, MD
[email protected]
Dear List Members,
I looked at the photos and B-scan of the case you posted today and was wondering what was going on in the superior orbit of this lady. There is a sausage-shaped low reflective area just behind the globe that almost looks a lot like an AV fistula. It doesn't look like it could be part of an oblique section of the optic nerve. I considered that possibility because the scan is labeled 12P. So the CT didn't notice anything unusual in this area, but did you do a longitudinal of 12? Maybe that would provide additional info about that area.
Best regards,
Cynthia Kendall
[email protected]
I looked at the photos and B-scan of the case you posted today and was wondering what was going on in the superior orbit of this lady. There is a sausage-shaped low reflective area just behind the globe that almost looks a lot like an AV fistula. It doesn't look like it could be part of an oblique section of the optic nerve. I considered that possibility because the scan is labeled 12P. So the CT didn't notice anything unusual in this area, but did you do a longitudinal of 12? Maybe that would provide additional info about that area.
Best regards,
Cynthia Kendall
[email protected]
Dear List Members,
I had a similar case about 10 years ago. It was 60 year old Korean female with what turned out to be a malignant melanoma. In the early stages, we could not diagnose the melanoma.
As in Dr. Finger's case:
1. The presumptive diagnosis is malignant melanoma.
2. I think a PET study will be helpful. It would not only give information about the lesion but also about the whole body, especially liver, lung, etc.
3. I think a biopsy is very dangerous. My recommendation is close observation (every month follow up). If it is malignant melanoma, it will grow rapidly. And you will find out the diagnosis within a few months.
4. If it is malignant melanoma (with the evidences of No. 2 and 3) then plaque radiotherapy should be employed.
Thank you,
Tai-Won Lee, MD
[email protected]
I had a similar case about 10 years ago. It was 60 year old Korean female with what turned out to be a malignant melanoma. In the early stages, we could not diagnose the melanoma.
As in Dr. Finger's case:
1. The presumptive diagnosis is malignant melanoma.
2. I think a PET study will be helpful. It would not only give information about the lesion but also about the whole body, especially liver, lung, etc.
3. I think a biopsy is very dangerous. My recommendation is close observation (every month follow up). If it is malignant melanoma, it will grow rapidly. And you will find out the diagnosis within a few months.
4. If it is malignant melanoma (with the evidences of No. 2 and 3) then plaque radiotherapy should be employed.
Thank you,
Tai-Won Lee, MD
[email protected]
DISCLAIMER: Postings on The ECN Mailing List are strictly the opinions of the authors. The ECN and its sponsors assume no responsibility for the accuracy of the information, nor do they assure the safety or effectiveness of any clinical recommendations in these postings.
Receive the latest news and opportunities from The Eye Cancer Foundation. Please fill out the form below.
Receive the latest news and opportunities from The Eye Cancer Foundation. Please fill out the form below.
