
Pediatric Unknown Intraocular Tumor Case 9
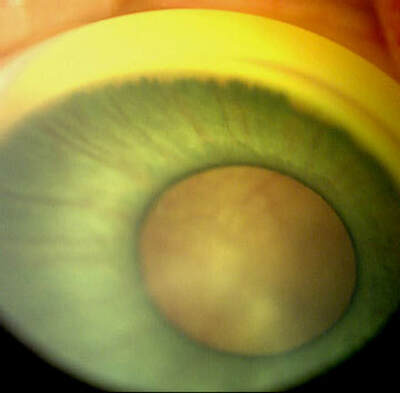
RetCam Digital Image
|
Subject: Unknown
Date: August 16th, 2002 Dear List Members We have a interesting case and would like to get your comments. Case This newborn presented with leukocoria due to a large creamy, white mass with fine overlying vessels occupying approximately two-thirds of the vitreous cavity OD. Normal retina and optic nerve could not be seen. The eye appeared small with a hypoplastic, greenish iris and persistent tunica vasculosa lentis but the anterior chamber was deep, angle open and the cornea and lens clear. (Retcam photo link below) Pregnancy and family history were unremarkable and the baby was otherwise normal. |
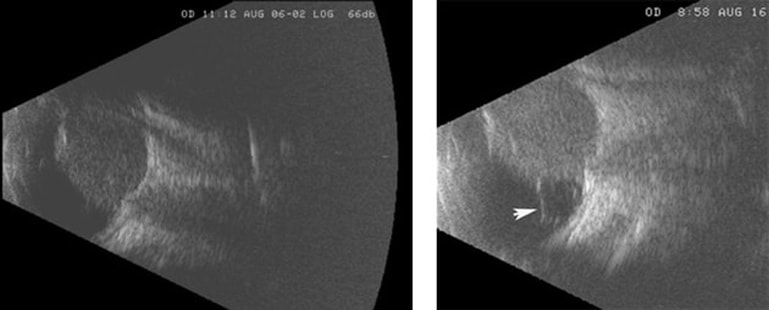
B-scan Ultrasonography - Note the homogeneous, non-calcified mass overlying the optic nerve and extending to the back surface of the lens. There is either a small retinal detachment or vitreous band (arrow) on the temporal side.
This is an active case and we would like to hear your comments and suggestions!
This is an active case and we would like to hear your comments and suggestions!
|
What will be your approach in this case?
Responses From ECN Members:Thank you for the great case. I would like to inquire about OS. Is there any tumor mass in the left eye? Is the eye of normal size or hypoplastic? Regarding OD, I think we are dealing with a dual pathology. First: a case of persistent fetal vasculature (PHPV) as evidenced by 1- microphthalmic eye ( the eye was small!!) 2- persistent iris vasculature as seen on the retcam picture 3- persistent tunica vasculosa lentis obscuring the view to the posterior pole 4- Persistent hyaloid system as could be demonstrated as a temporal vitreous band on US, and a band nicely seen on T2-weighted coronal view on MRI. |

Computed Axial Tomography - CT without contrast showed a small, abnormally shaped eye, squared off posteriorly with an area of irregular, thinned or deficient sclera posteronasally (arrow). The mass was not calcified and enhanced minimally with contrast.
|
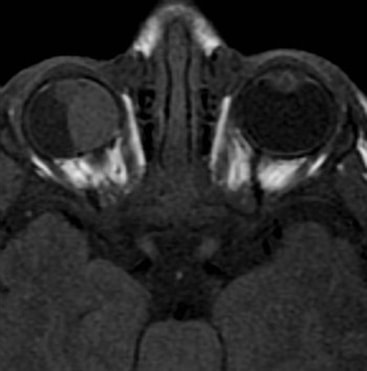
Magnetic Resonance Imaging - Axial MRI shows the homogeneous mass, isodense with brain, in the misshapen eye. The lens appears spherical.
|
Second: a case of exophyticretinoblastoma, presented as a soft tissue mass with absent calcification ( a finding in 20 % of cases or Rb). The mass is compressing the sclera and may be even infiltrating it as seen on CT and MRI. Comparing CT and MRI indicates the presence of an overlying RD. Also, the soft tissue mass has the intensity of intraocular Rb on MRI.
Regarding management, enucleation would be a reasonable approach as the eye is non-seeing with high chances of harboring retinoblastoma. I would be very cautious in enucleation to open the globe and disperse tumor cells everywhere while applying traction on the medial rectus to cut ON. I would use an optic nerve snare or a spoon to lift the globe rather than pull on it. |
|
Of course, it is very important to cautiously look on pathology specimen to see any invasion to optic nerve, choroid, or sclera. This would warrant additional treatment. Sincerely, Ihab Saad Othman, MD, FRCS Consultant Ophthalmic Surgeon Cairo University [email protected] |
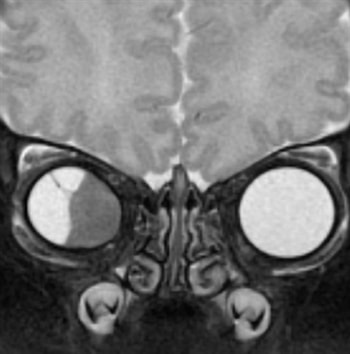
Magnetic Resonance Imaging - Coronal T2 weighted MRI confirms the mass is not blood and does not contain melanin. The border of the mass is smooth and a band extends to the superotemporal sclera (arrow). The nasal sclera is thinned and the eye “egg shaped.”
|
Brenda Gallie has presented an interesting case. There is definitely PHPV and a tumoral mass that is too large to be just PHPV. Retinoblastoma is not associated with PHPV. I reported a case with retinoblastoma and PHPV in opposite eyes and there is only one report of PHPV and retinoblastoma in the same eye. The tumor that is most frequently associated with PHPV is medulloepithelioma. If this is a medulloepithelioma, it is most likely a malignant medulloepithelioma, because of the invasion of the uvea and possibly sclera. I would recommend enucleation.
Ian W. McLean, MD
Ophthalmic Pathology
Armed Forces Institute of Pathology
Washington, DC 20306-6000
[email protected]
Ian W. McLean, MD
Ophthalmic Pathology
Armed Forces Institute of Pathology
Washington, DC 20306-6000
[email protected]
I do not think that this is RB - although some small or diffuse RB tumours have minimal or no calcification, a tumour this large would show evidence of calcification on US / CT. A malignant medulloepithelioma is a distinct possibility and I would have no hesitation in recommending enucleation in this abnormal eye with no visual potential.
James Muecke, MD
The Department of Ophthalmology
Royal Adelaide Hospital, Australia
61-8-8222-5222
[email protected]
James Muecke, MD
The Department of Ophthalmology
Royal Adelaide Hospital, Australia
61-8-8222-5222
[email protected]
DISCLAIMER: Postings on The ECN Mailing List are strictly the opinions of the authors. The ECN and its sponsors assume no responsibility for the accuracy of the information, nor do they assure the safety or effectiveness of any clinical recommendations in these postings.
Receive the latest news and opportunities from The Eye Cancer Foundation. Please fill out the form below.
Receive the latest news and opportunities from The Eye Cancer Foundation. Please fill out the form below.
